Overview
Cervicogenic headache is a distinct type of headache that occurs when pain is referred from a specific source in the neck up to the head. This is characterized by a dull, non-throbbing pain that radiates from the neck to back of the head. The pain may spread along the scalp and affect the forehead, temple, and area around the eye and/or ear. Cervicogenic headache is caused due to an underlying joint, disc, muscle, or nerve disorder in the neck. The upper cervical facet joints relating to vertebrae C1-C3 are most commonly involved in cervicogenic headache pain.
Anatomy (Neck Anatomy)
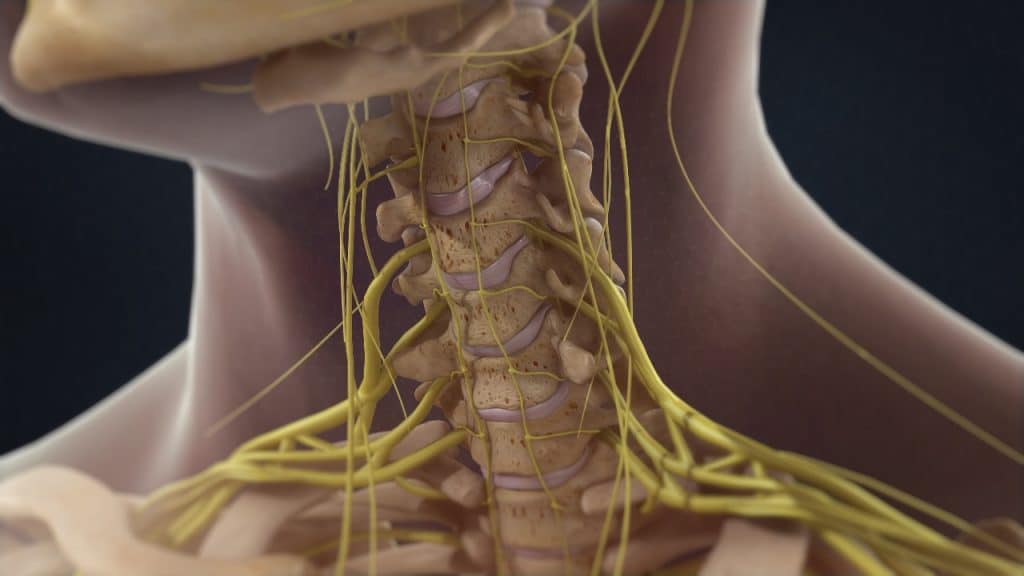
Neck anatomy is a well-engineered structure of bones (vertebrae), nerves, muscles, ligaments and tendons. The cervical spine consists of seven vertebrae, which are the smallest and uppermost in location within the spinal column and supported by strong ligaments and several muscles. The cervical vertebrae connect the neck to the thoracic spine (the upper back). All seven vertebrae are numbered. The C1, the first vertebra in the column (closest to the skull), is also known as the atlas. The C2, the vertebra below it, is also known as the axis. The C stands for cervical.
Anatomy (The Atlanto-Occipital Joint)
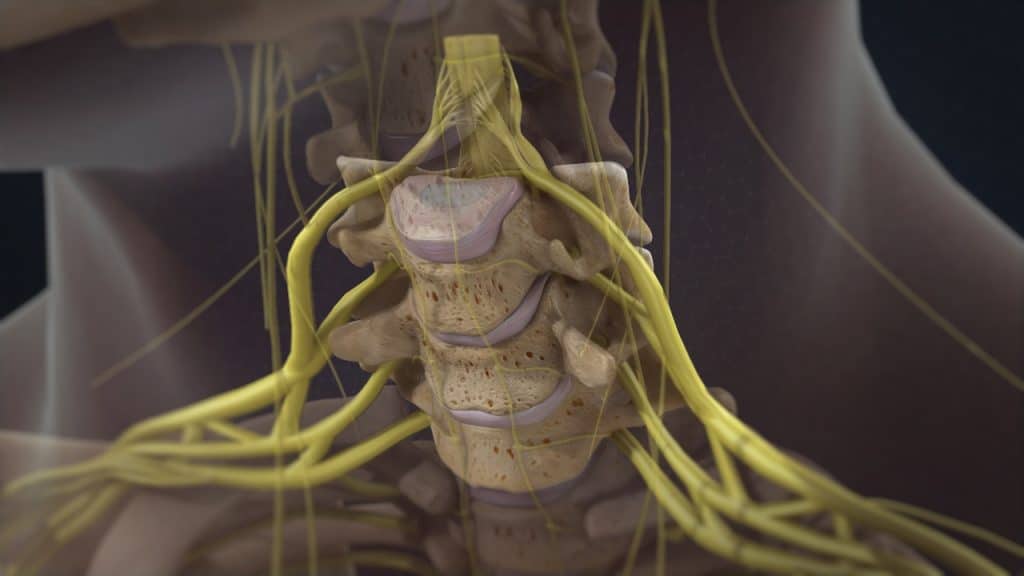
This joint is where the lower part of the occipital bone (base of the skull) connects with the first cervical vertebra, called the atlas. This region facilitates the passing of the spinal cord out of the skull and down into the cervical spine.
Anatomy (Intervertebral Discs)
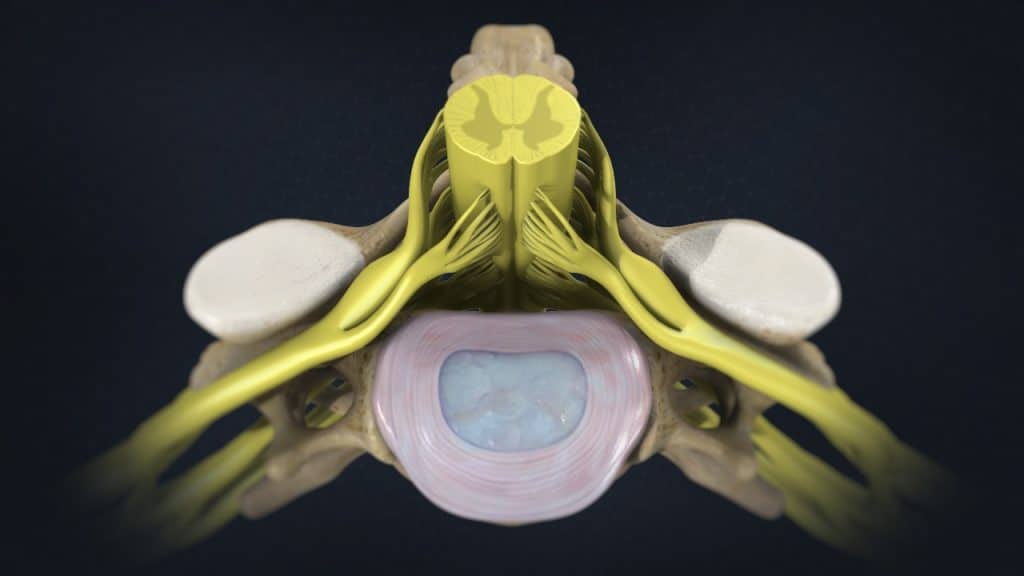
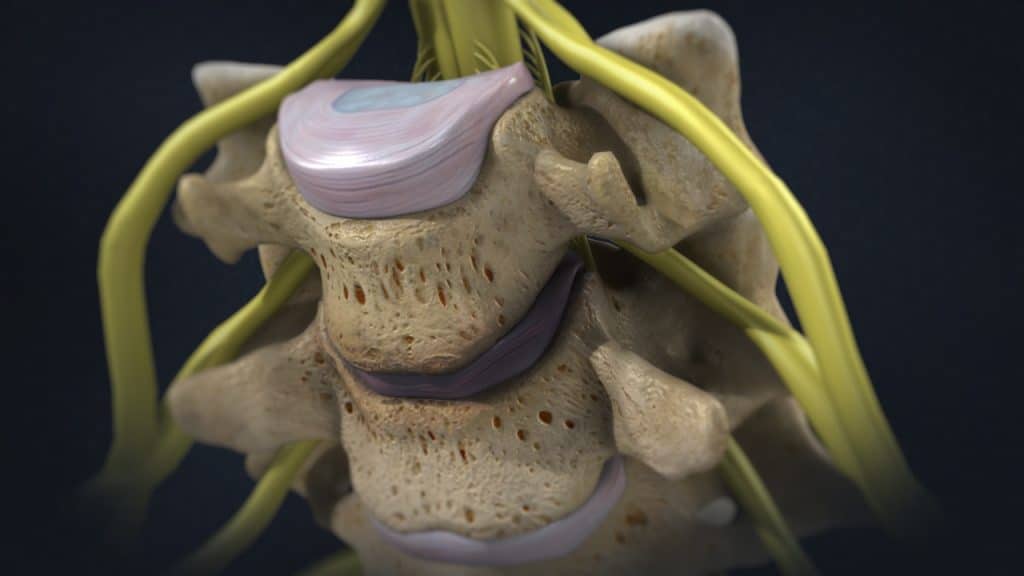
The intervertebral discs are shock absorbers that are located between the bones of the spine, called vertebrae (hence the name intervertebral). They are designed to help the back stay flexible while resisting forces and to allow bending, flexion and twisting of the spine. Each disc has a thick outer layer, known as annulus fibrosus, that surrounds the soft gel-like center, known as nucleus pulposus. A herniated disc occurs when the jelly-like material inside the disc nucleus herniates or leaks out of the disc, and presses on an adjacent nerve root.
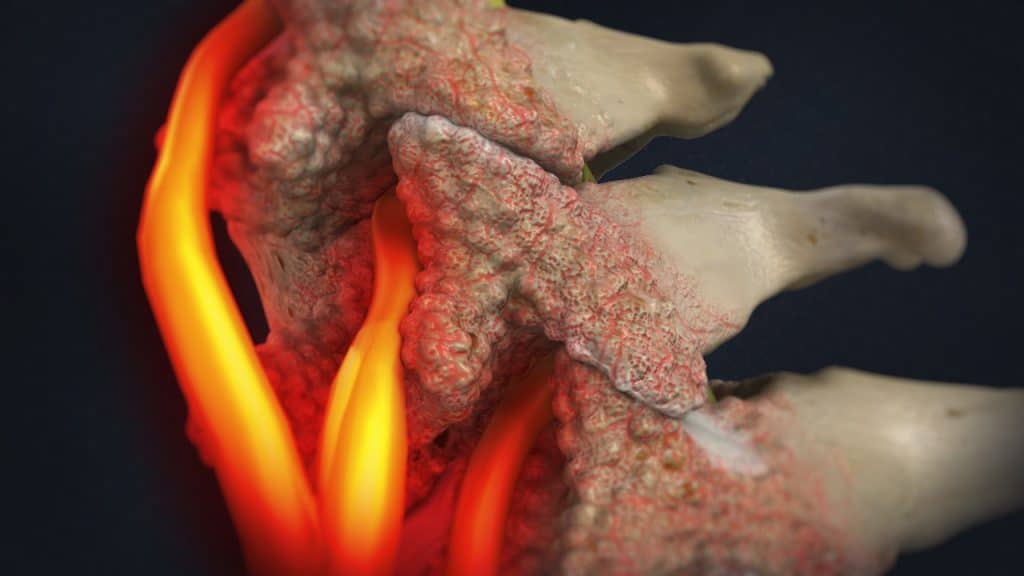
Anatomy (Facet Joints)
The facet joints or zygapophyseal joints are a set of joints between the articular processes of two adjacent vertebrae. They are covered with cartilage and are surrounded by a lubricating capsule that enables the vertebrae to bend and twist. Each capsule has a rich supply of tiny nociceptive nerve fibers and implicates this structure as a potential source of pain. Similar to other joints in the body, the facet joints are vulnerable to inflammation and degeneration.
Causes
The causes for cervicogenic headache are based on the involvement of several anatomical structures in the upper cervical region that are sensitive to pain. The nerves that supply these structures are capable of referring pain from the neck to different parts of the head, including the forehead, temple, eye and ear. Cervicogenic headache is caused due to an underlying joint, disc, muscle, or nerve disorder in the neck. The anatomical structures within the cervical region are interconnected, so an injury to one is likely to affect the health of the others.
Causes (Trauma)
Cervicogenic headache can be caused by direct trauma to the back of the head or neck. This could be anything from a fall to a car accident or even a sports injury. The facet joints in the cervical spine are prone to injury due to the weight-bearing function they perform while supporting the head. The most common cause of trauma to facet joints is whiplash injury as a result of a motor vehicle accident, resulting in pain shortly after the injury. Cervicogenic headache originating from whiplash may resolve in a few days or may last for years. An injury to the atlanto-occipital joint can trigger cervicogenic headache as well.
Causes (Facet Joint Disease)
Facet joint syndrome or facet joint disease is a pain arising from the intervertebral joint facets.
Similar to other joints in the body, the facet joints are vulnerable to inflammation and degeneration. The upper cervical facet joints relating to vertebrae C1-C3 are most commonly involved in cervicogenic headache pain, although the facet joints of lower cervical vertebrae can be also involved.
Causes (Degenerative Disc Disease)
Degenerative disc disease is an age-related condition that happens when one or more of the discs deteriorate or break down, leading to pain.
Causes (Cervical Herniated Disc)
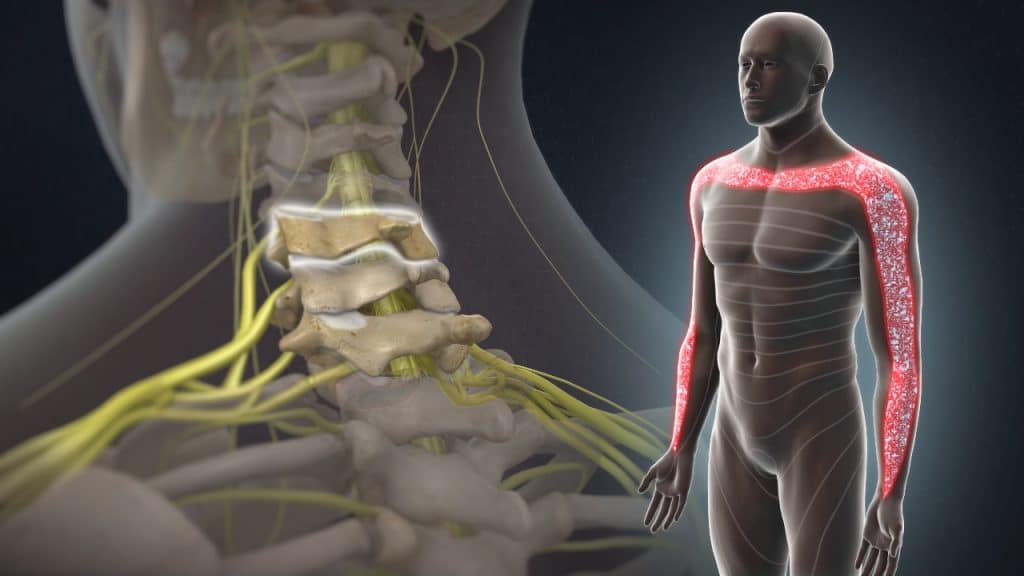
Cervical disc herniation is a disease affecting the neck that may trigger cervicogenic headache. A herniated disc can allow disc material to press harmfully against nearby nerve roots, triggering neck pain and possibly pain and nerve symptoms such as tingling, numbness, and/or weakness that can radiate down into the shoulder, arm, and/or hand.
Causes (Cervical Radiculopathy)
Cervical radiculopathy is a disease involving dysfunction of one or more nerve roots in the cervical spine that typically manifests as pain radiating from the neck into the distribution of the affected nerve root. It can be accompanied by sensory, motor, or reflex disturbances. Any condition that somehow compresses or irritates a cervical nerve root can cause cervical radiculopathy. It most often results from degenerative disease in the cervical spine, but it can also occur due to an acute injury or illness. Patients with cervical radiculopathy, especially in the upper spinal region may develop cervicogenic headache as well.
Causes (Injury to the Spinal Nerves)
Compression and irritation of cervical spinal nerves can trigger cervicogenic headache. The nerves that innervate the most commonly affected facet joint, C2-C3, in cervicogenic headache are medial branches that continue their path to become the third occipital nerve. This nerve continues to course around the back of the head and around the scalp, which is the path followed by cervicogenic headache pain.
Causes (Injury to the Neck Muscles)
Overuse or disuse of certain neck muscles may result in muscle fatigue or weakness leading to cervicogenic headache. People who constantly sit with their head in forward and/or downward positions, such as those who do computer jobs on a continual basis, can end up with tight muscles at the back of the head, and eventually can develop cervicogenic headache.
Furthermore, certain occupations such as hair stylists and drivers may be at a higher risk for cervicogenic headache due to their head posture while working.
Symptoms
Cervicogenic headache is characterized by dull, non-throbbing pain of mild or moderate intensity that radiates from the neck to the back of the head. The pain may spread along the scalp and affect the forehead, temple, and area around the eye and/or ear. It usually affects only one side of the head, but in severe cases can be experienced on both sides. Cervicogenic headache symptoms may be aggravated by certain activities or postures and may also be accompanied by some neck stiffness and reduced range of motion. Pain in the shoulder and/or arm of the affected side and pain between the shoulder blades, especially by irritation of the lower cervical motion segments, is also common. Blurring of vision may be felt in the eye of the affected side in some cases as well.
Treatment
Treatment of cervicogenic headache focuses on the underlying condition to control symptoms. There is no specific treatment protocol for cervicogenic headache, and a combination of different techniques may be required to alleviate the pain.
Treatment for the cervicogenic headache is mainly conservative with rest, heat therapy, analgesic/anti-inflammatory medications, muscle relaxants, manual and physical therapy. Moreover, a transcutaneous electrical nerve stimulation (TENS) may be administered. This stimulates the sensory nerves, creating a tingling sensation in the area, thereby reducing the feeling of pain.
Facet joint infiltrations or facet joint blocks may be administered not only to diagnose facet joint pain but also to treat it. If the patient shows a positive response to the facet joint blocks after having failed nonoperative care, the next treatment option is often radiofrequency denervation or rhizotomy.
The cervical radiculopathy can usually be treated successfully without surgery with a combination of pain management techniques, physical therapy and therapeutic spinal injections.
Surgery may be recommended if the conservative therapies do not alleviate pain or if a significant neurologic deficit such as progressive muscle weakness or compression on the cervical spinal cord, known as cervical myelopathy, exists.
References
- Kraemer J., Hasenbring M., Kraemer R., Taub E., Theodoridis T., Wilke H.J.: Intervertebral Disc Diseases: Causes, Diagnosis, Treatment and Prophylaxis. Thieme 2009.
- Haldeman S., Dagenais S.: Cervicogenic Headaches. A critical Review. The Spine Journal 2001; 1(1): 31-46.