Overview
Numerous studies in the medical literature have shown that the herniated disc has the potential for spontaneous regression or disappearance. Although some patients need surgical intervention because of prolonged intolerable pain, the majority of them heal spontaneously without surgery. Furthermore, several studies in the past years indicate that early surgery achieves more rapid relief of herniated disc symptoms than conservative care – but, in the long run, outcomes gradually become identical to conservative treatments.
Different forms of nonsurgical treatments should be exhausted before considering surgery in acute stages of herniated disc.
Surgery may be recommended if the conservative therapies do not alleviate the pain or if a significant neurologic deficit – such as progressive muscle weakness – exists.
Disc Anatomy
The intervertebral discs are shock absorbers that are located between the bones of the spine. Those are called vertebrae (hence the name intervertebral). They are designed to help the back stay flexible while resisting forces and to allow bending, flexion and twisting of the spine. Each disc has a thick outer layer, known as annulus fibrosus, that surrounds the soft gel-like center, known as nucleus pulposus.
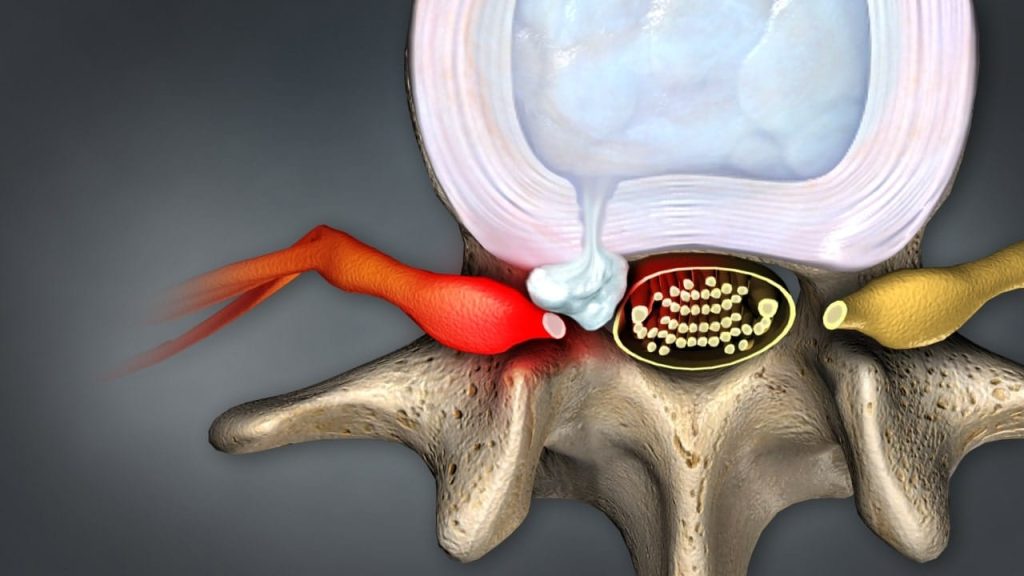
Herniated Disc
A herniated disc occurs when the jelly-like material inside the disc nucleus herniates or leaks out of the disc that can press on an adjacent nerve root.
Lumbar disc herniation is a disease affecting the lower back.
Cervical disc herniation is a disease affecting the neck.
Types of Spinal Disc Herniation
A disc protrusion refers to bulging of the disc in which the annulus fibrosus remains intact.
A disc prolapse is a condition in which the annulus fibrosus is perforated, disc tissue penetrates it and leaks out of the inside of the disc.
A disc extrusion occurs when the nucleus squeezes through a weakness or tear in the annulus, but the soft material is still connected to the disc.
A disc sequestration is a subtype of extrusion occurring when the nucleus not only squeezes out but separates from the main part of the disc. This is also known as a free fragment.
Causes
Α herniated disc commonly results from age-related weakening of the intervertebral disc, known as degenerative disc disease. It can occur gradually over many years as a result of normal wear and tear on the spine, such as constant sitting or squatting, driving, or a sedentary lifestyle. A herniated disc can also be caused by heavy lifting or by sudden, damaging motions, such as abrupt bending or torsional movements of the lower back. It can also be traumatic in origin.
Symptoms
Symptoms of a herniated disc vary depending on the location of the affected disc and the severity of the rupture. An affected disc in the lower back may result in pain in the back, buttock, or leg, while an affected disc in the neck area may result in neck or arm pain. The pain often gets worse with movements such as bending, twisting, lifting and sitting.
Possible Mechanisms of Spontaneous Disc Regression
The exact mechanism of spontaneous disc regression remains unknown. Three popular theories are present in the literature. It is possible that one specific or different combinations of the following three mechanisms may play a role in spontaneous regression of the herniated disc tissue:
1. Gradual degradation and shrinkage of the disc
The herniated disc fragment reduces in size due to gradual dehydration and shrinkage.
2. Retraction of the herniated disc back
The herniated disc fragment retracts back into the intervertebral space due to the tension applied by the posterior longitudinal ligament (a very strong ligament which forms the anterior wall of the vertebral canal). This mechanism may explain the cases where the herniated disc fragment has an intact annulus fibrosus, but not the cases with completely extruded or migrated disc fragments.
3. Enzymatic degradation – phagocytosis – neovascularisation
The intervertebral disc is the largest avascular (lack of blood vessels) organ in the human body and considered an immune-privileged site.
This theory states enzymatic degradation and macrophage phagocytosis of the extruded disc material due to inflammatory reaction and neovascularisation. (Phagocytosis is a process by which certain living cells ingest or engulf other cells or particles).
This is the most recognisable mechanism. It describes an inflammatory reaction where the autoimmune system of the body recognizes the extruded disc tissue as a “foreign body” in the epidural vascular space of the vertebra. This causes neovascularisation (proliferation of the blood vessels) of the disc material and infiltration by inflammatory cells such as macrophages, granulocytes, and lymphocytes. Macrophages are indicated as the most important immune players in the resorption process of herniated discs.
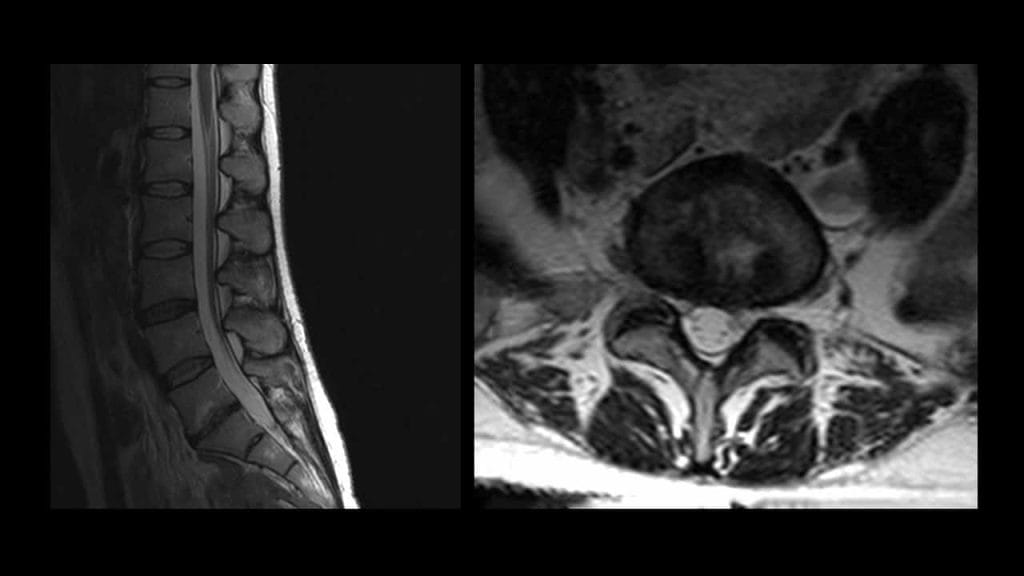
Features of Magnetic Resonance Imaging (MRI)
Magnetic resonance imaging (MRI) is a current technique to document the regression of herniated intervertebral disc fragments.
Several studies with lumbar MRI have demonstrated that the largest the lumbar disc herniations are most likely to show the greatest regression in size over time. Furthermore, disappearance of herniated disc material is seen frequently in the cases of migrating/sequestered disc herniation. Many studies have reported that the more the disc tissue migrated, the greater the subsequent decrease in size that could be observed.
Spontaneous regression time is not clear. It has been reported that the regression usually occurs between three months and one year.
Conservative versus Surgical Treatment
The current treatments for herniated disc can be divided into conservative versus surgical approaches and the decision on which approach to use, is variable and patient-clinician dependent.
Numerous studies have reported excellent recovery of herniated disc symptoms with non-operative treatment. Furthermore, several studies in the past years indicate that early surgery achieves more rapid relief of herniated disc symptoms than conservative care. But, in the long run, outcomes gradually become identical to conservative treatment.
Different forms of nonsurgical treatments should be exhausted before considering surgery in acute stages of herniated discs. These include pain management techniques, physical therapy and therapeutic spinal injections.
Surgery may be recommended by prolonged intolerable pain despite the conservative therapies. It is clear that the surgery should be the first choice of treatment if a significant neurologic deficit – such as progressive muscle weakness – exists. Cauda equina syndrome is a medical emergency that calls for urgent surgical intervention. Most cases of myelopathy will require an operation to relieve pressure on the spinal cord.
References
- Kraemer J., Hasenbring M., Kraemer R., Taub E., Theodoridis T., Wilke H.J.: Intervertebral Disc Diseases: Causes, Diagnosis, Treatment and Prophylaxis. Thieme 2009.
- Kraemer J., Koester O.: MR Imaging of the Lumbar Spine. A Teaching Atlas. Thieme 2002.
- Cunha C., Silva A., Pereira P., Vaz R., Goncalves R., Barbosa M.: The inflammatory response in the regression of lumbar disc herniation. Arthritis Research & Therapy 2018 Nov 6; 20 (1):251. doi: 10.1186/s13075-018-1743-4.
- Fager C.: Observations on spontaneous recovery from intervertebral disc herniation. Surg Neurol 1994; 42:282-286.
- Komori H., Shinomiya K., Nakai O., Yamaura I., Takeda S. Furuya K. The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996; 21(2):225-229.
- Chang C. Lai P., Yip C., Hsu S.: Spontaneous regression of lumbar herniated disc. Journal Chin Med Assoc 2009; 72 (12): 650-653.
- Hahne AJ., Ford JJ., McMeeken JM.: Conservative management of lumbar disc herniation with associated radiculopathy: a systemic review. Spine 2010; 35(11): E488-E504.
- Jacobs W., Tulder M., Arts M., Rubinstein S., Middelkoop M., Ostelo R., et.al.: Surgery versus conservative treatment of sciatica due to a lumbar herniated disc: a systemic review. Eur Spine Journal 2011; 20(5): 513-522.
- Lurie JD., Tosteson TD., Tosteson AN., Zhao W., Morgan TS., Abdu WA, et al.: Surgical versus nonoperative treatment for lumbar disc herniation; eight-year results for the Spine Patient Outcomes Research Trial. Spine 2014; 39(1): 3-16.