Overview
A compression fracture occurs when the vertebral bone (bone of the spine) collapses. It usually occurs in the middle and lower part of the thoracic spine and in the upper part of the lumbar spine.
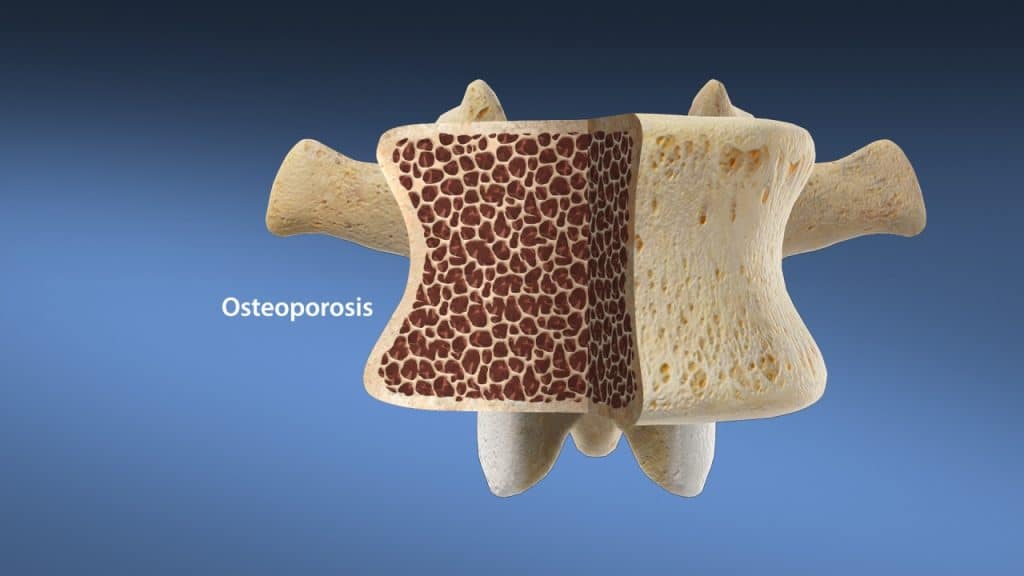
Compression fractures are most commonly caused by osteoporosis in elderly and postmenopausal women. Osteoporosis is characterized by loss of bone density and impaired bone microarchitecture resulting in bones that are brittle and liable to fracture. Compression of these vulnerable vertebrae leads to small fractures in the front of the vertebral bone (wedge deformation), in the middle part (concave or biconcave deformation) or vertebral body collapse. Bone compression results in height loss of the osteoporotic vertebra, which can cause upper οr lower back pain and postural changes.
Anatomy (Thoracic region)
The thoracic spine is located in the upper back and is the longest region of the spine. The thoracic spine consists of twelve vertebrae, labelled from T1 down to T12. T stands for thoracic. T1, the top thoracic vertebra, connects with the lowest cervical vertebra, C7, in the cervical spine above, while the lowest thoracic vertebra, T12, with the first lumbar vertebra, L1, in the lumbar spine below. Additionally, these vertebrae serve as attachment points for the ribcage. The costovertebral joints are where the thoracic vertebrae connect or articulate with the ribs.
Anatomy (Lumbar region)
The lumbar spine consists of five vertebrae which connect the sacrum (triangular bone at the bottom of the spine) to the thoracic spine (the upper back). All five vertebrae are numbered. L1, the first lumbar vertebra, is closest to the thoracic spine. L5, the lowest lumbar vertebra, is closest to the sacrum. L stands for lumbar.
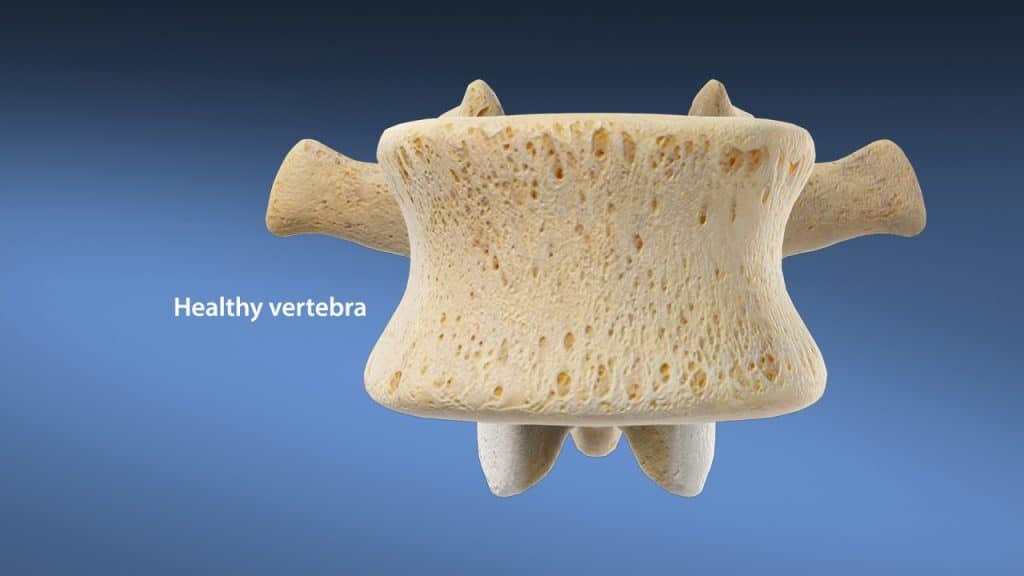
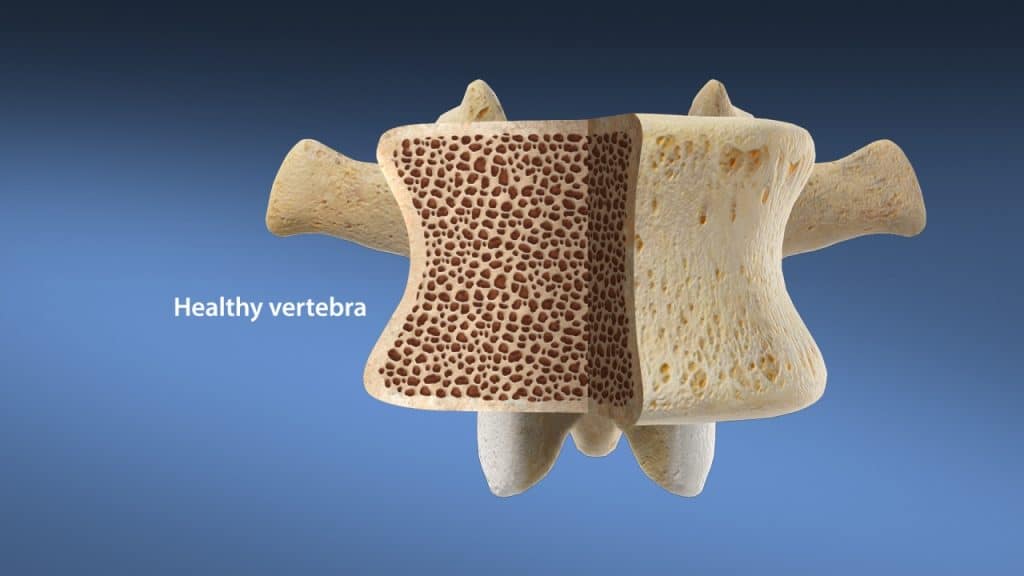
Anatomy (A typical lumbar vertebra)
A typical lumbar vertebra (bone of the spine) is composed of two parts. The vertebral body in the front (anterior) and the vertebral arch in the rear (posterior).
The vertebral arch encloses the vertebral foramen (opening). It consists of a pair of pedicles and a pair of laminae. At the junction of the pedicle and lamina on the right and left side, bony protrusions project upward and downward, known as superior and inferior articular processes.
The pars interarticularis (bridge between two bones) connects the superior and inferior articular processes. The pars interarticularis may also be referred to as the isthmus.
At the mid-point of the vertebral arch, a bony protrusion known as spinous process projects backward and downward. On either side of the spinous process, there are bony protrusions known as transverse processes. Similar to the spinous process, these processes provide attachments for ligaments and muscles. The vertebrae (bones of the spine) articulate with one another at joints between their bodies and between their articular processes. The intervertebral discs provide the strongest attachment between the bodies of the vertebrae. In addition to the discs, the bodies are united by strong supporting ligaments.
Common Cause (Osteoporosis)
Osteoporosis is associated with loss of bone density and impaired bone microarchitecture resulting in bones that are brittle and liable to fracture. It is by far the most common cause of compression fractures of the spine, especially in postmenopausal women. Depending on the severity of the osteoporosis, the compression fractures can occur after a minor trauma or stress to the spine or in advanced cases non-traumatic during coughing or sneezing.
Symptoms
The first symptom of a compression fracture due to osteoporosis is mostly a severe acute back pain which is often relieved by rest. The area around the fracture is tender to palpation and pressure. This pain usually gets better after 6-12 weeks as the bone heals. By some patients, however, the pain can persist due to myofascial irritation as a result from postural changes, inappropriate biomechanical stress and inactivity.
Multiple compression fractures (fracture of more than one vertebra) can lead to kyphosis. Kyphosis is the general term used to define any excessive forward curvature of the thoracic spine, causing hunching of the back. Furthermore, a person who experiences multiple compression fractures may notice a loss of height.
The compression fractures of the spine are usually stable and rarely accompanied by any nerve or spinal cord damage. If this is the case, an affected spinal nerve may result in back pain and possibly pain and nerve symptoms such as tingling, numbness and/or weakness that can radiate in the area supplied by the affected nerve root. Furthermore, in rare cases, the severe compression on the nerve bundle at the end of the spinal cord, known as cauda equina (horse’s tail) can lead to serious neurological disorders such as a loss of bowel or bladder function, a condition known as cauda equina syndrome. The spinal cord compression in the thoracic spine can also lead to severe neurological deficits such as extreme weakness, disorders of balance and coordination or even paralysis, a condition known as thoracic myelopathy.
Treatment
Conservative management is the traditional first-line therapy for compression fractures of the spine. It comprises both treatment of the fracture and treatment of the underlying osteoporosis.
The treatment may include rest, heat- or cryotherapy, analgesic/anti-inflammatory medications and physical therapy. The wearing of back brace for approximately 3 months is highly recommended in order to support the back. It prevents bending forward and therefore removes pressure from the injured vertebra and helps to avoid progressive kyphosis and respiratory impairment. The compression fracture of the spine usually takes about 3 months to fully heal.
Surgical treatment is indicated in cases of unstable fractures, strong pain despite conservative therapy and progressive height loss of the vertebrae with increasing kyphosis. The usual surgical techniques are vertebroplasty and kyphoplasty. These minimally invasive procedures are designed to inject a cement mixture into the fractured vertebra in order to stabilize the bone, eliminate pain and prevent a spinal deformity from progressing.
Spinal fusion surgery (spondylodesis) may be recommended if the fracture is considered unstable or if a significant neurologic deficit such as progressive muscle weakness or compression on the thoracic spinal cord, known as thoracic myelopathy, or compression on the cauda equina, known as cauda syndrome, exists.
In order to avoid further fractures, the treatment of the underlying osteoporosis is mandatory. This includes lifestyle recommendations to prevent from further bone loss and fractures and to strengthen the bone structure. Moreover, in most cases a specific medication that works at cellular level to avoid further bone resorption and promote bone formation is indicated.
References
- Niethard F., Pfeil J., Biberhaler P.: Orthopädie und Unfallchirurgie. 6. Auflage. Thieme 2009.
- Wirth CJ., Mutscher W.: Praxis der Orthopädie und Unfallchirurgie. 2. Auflage. Thieme 2009.
- Moore K.: Clinically Oriented Anatomy. Third Edition. Williams & Wilkins 1992.
- Solomon L., Warwick D., Nayagam S.: Apley’s System of Orthopaedics and Fractures. Hodder Arnold 2001.
- Kraemer R., Theodoridis T., Kraemer J.: Die lumbale Spinalkanalstenose. Springer 2011.