Overview
Spondylolisthesis occurs when one vertebra slips over the adjacent one and is a common cause of low back pain. It slides either forward (anterolisthesis) or backward (retrolisthesis). Spondylolisthesis has a variety of causes. This condition is commonly caused by mechanical instability of the facet joints as a result of degenerative conditions such as osteoarthritis and/or degenerative disc disease. Degenerative spondylolisthesis typically occurs at the L4-L5 level of the lumbar spine and it mostly affects people over 50. The symptoms of degenerative spondylolisthesis are very commonly the same as those of spinal stenosis. This may cause pain, tingling, numbness and/or weakness that radiates from the lower back into the buttocks and legs in the area supplied by the affected nerve root.
Anatomy (Intervertebral discs)
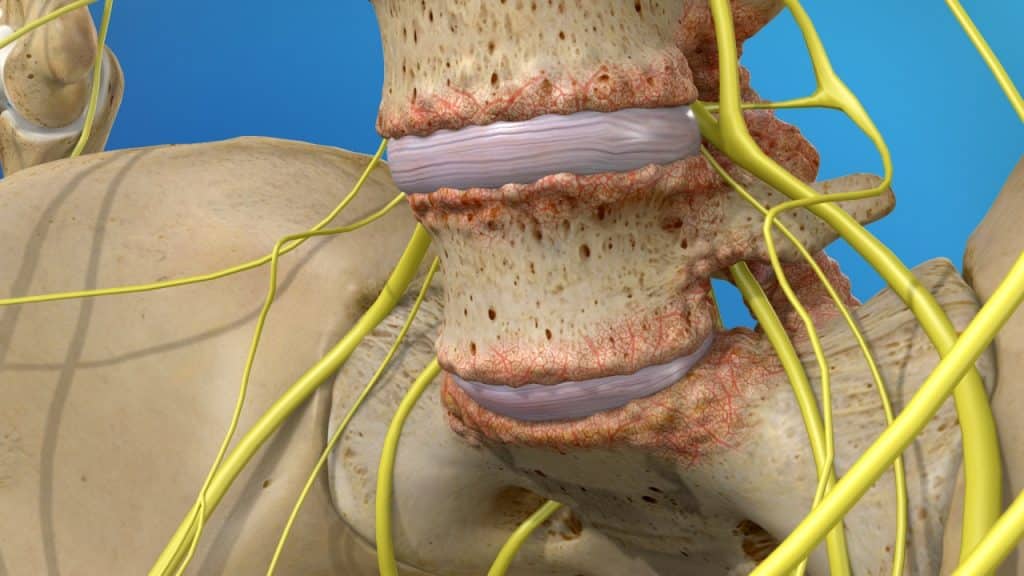
The intervertebral discs are shock absorbers that are located between the bones of the spine, called vertebrae (hence the name intervertebral). They are designed to help the back stay flexible, while resisting forces and to allow bending, flexion and twisting of the spine. A healthy, well-hydrated disc contains a great amount of fluid in its centre, known as the nucleus pulposus, which provides cushioning and flexibility to the spine.
Anatomy (Facet joints)
The facet joints or zygapophyseal joints are a set of joints between the articular processes of two adjacent vertebrae. They are covered with cartilage and are surrounded by a lubricating capsule that enables the vertebrae to bend and twist. Each capsule has a rich supply of tiny nociceptive nerve fibers and implicates this structure as a potential source of pain. Similar to other joints in the body, these joints are vulnerable to inflammation and degeneration.
The facet joints provide support, stability and mobility to the vertebrae, especially on extending, bending and rotation. Furthermore, the articulation between the superior (above) and inferior (below) articular facets at the zygapophyseal joints as well as the intervertebral discs play an important role to prevent a vertebra slip over the adjacent one.
Degenerative spondylolisthesis occurs as a consequence of the general aging process in which the bones, joints and ligaments in the spine become weak and less able to hold the spinal column in alignment.
Degeneration Process
The degeneration process usually begins with the discs – Disc Degeneration:
1.Loss of Fluid
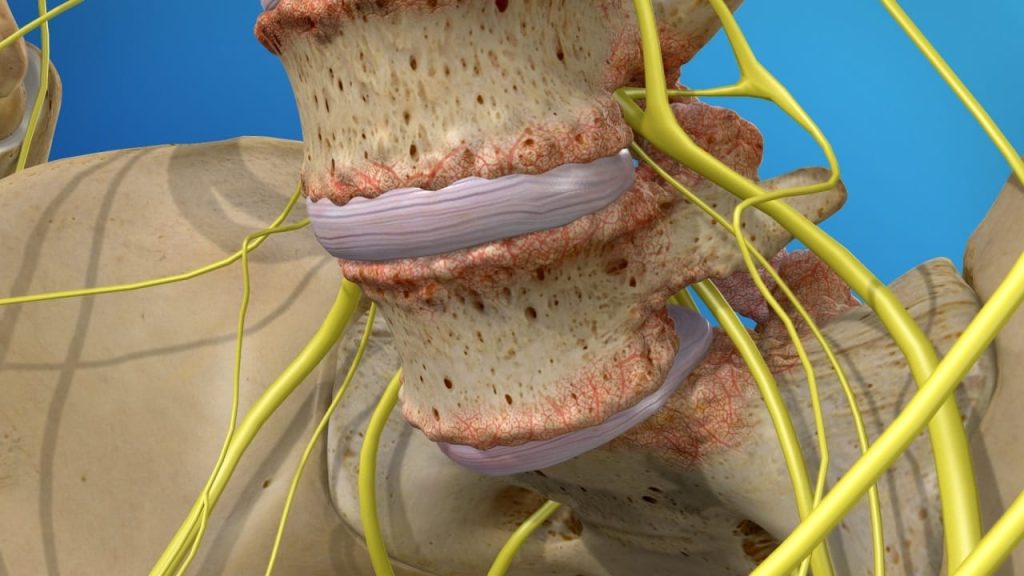
A degenerated disc is marked by a significant decrease in hydration, making the disc less flexible, thinner with narrowing the distance between the adjacent vertebrae, and more prone to tearing or cracking in the outer layer of the disc (disc wall), known as annulus fibrosus.
2. Disc Tearing – Disc Healing – Disc Weakening and Collapse
The disc is unable to truly repair itself because it does not have a direct blood supply. Consequently, a tear in the annulus either will not heal or will develop a scar tissue that is not as strong as the original one, having the potential to break again with further disc-weakening and collapse.
3. Breakdown of Cartilage between the Facet joints – Facet Joint Disease
As the space between the two vertebrae above and below the affected disc gets smaller, there is less padding between them, and the spine becomes less stable. The facet joints, the areas where the vertebrae touch, are forced to shift which can affect their function. The cartilage that covers the stressed facet joints gradually wears away. The joints become swollen and stiff. The vertebral bones rub directly against each other, which can lead to growth of bone spurs along the edges of the facet joints and an enlargement of the joints. Facet joint disease occurs when these joints become stressed and damaged.
4. Bone Spurs Formation
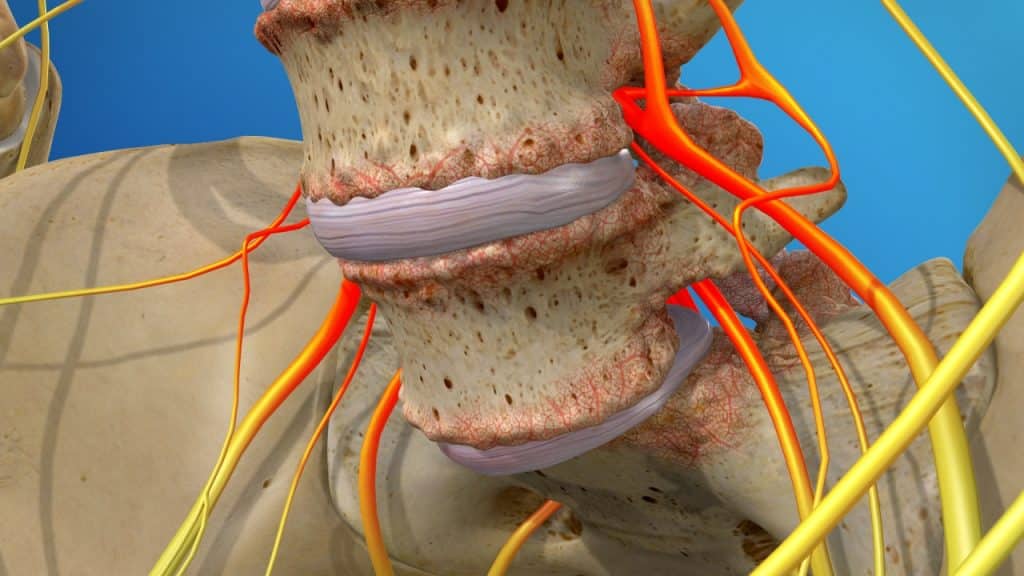
Furthermore, the body can react to the closing gap between the two vertebrae by building osteophytes or bone spurs, small bony projections that develop along the edges of bones. Bone spurs can put pressure on the spinal nerve roots or spinal cord, resulting in pain and affecting nerve function.
5. Spinal Stenosis
The vertebral shifting and the excess growth of bone (bone spurs or osteophytes) can reduce the space through which the nerve roots travel, and the spinal cord or the nerve roots can become harmfully compressed.
Symptoms
Degenerative spondylolisthesis may be asymptomatic. The symptoms can be experienced in a variety of ways. Low back pain can be mild or so intense that the individual cannot follow everyday activities. It can occur suddenly or develop slowly and gradually aggravate over time. Low back pain usually gets worse after prolonged standing and is often relieved by rest.
Patients typically have tight hamstring muscles (the muscles in the back of the thigh), reduced flexibility in the lower back and difficulty or pain when bending backwards.
The pain arising from the facet joints may be experienced in the lower back with radiation into the buttocks, groin, lower abdomen and back of the thigh.
Generally, spinal stenosis symptoms develop slowly over time and they tend to recur. They usually occur during certain activities such as walking (painful cramping or weakness in the legs during walking, known as neurogenic claudication) and prolonged upright standing (in the upright position the spinal canal gets narrower, worsening the stenosis and pitching the nerve roots in the canal). The symptoms are often relieved by rest (sitting or lying down) and/or any flexed forward posture, which opens up the spinal canal. Spinal stenosis in the lower back commonly causes pain, tingling, numbness and/or weakness that radiates from the lower back into the buttocks and legs in the area supplied by the affected nerve root.
Treatment
Treatment for painful spondylolisthesis focuses on minimizing pain, stabilizing the spine and improving or maintaining mobility. It can usually be treated successfully without surgery with a combination of rest, step positioning (stress-reducing positioning), heat therapy, analgesic/anti-inflammatory medications, orthopaedic braces and physical therapy.
Facet joint infiltrations or facet joint blocks may be administered not only to diagnose facet joint pain but also to treat it. If the patient shows a positive response to the facet joint blocks after having failed nonoperative care, the next treatment option is often radiofrequency denervation or rhizotomy.
The spinal stenosis can usually be treated successfully without surgery with a combination of pain management techniques, physical therapy and therapeutic spinal injections. Surgery may be recommended if the conservative therapies do not alleviate pain and the quality of life is still affected or if a significant neurologic deficit such as progressive muscle weakness exists. Surgery for degenerative spondylolisthesis usually includes a decompression (also called a laminectomy) with or without spinal fusion with pedicle screw instrumentation (spondylodesis).
References
- Kraemer J., Hasenbring M., Kraemer R., Taub E., Theodoridis T., Wilke H.J.: Intervertebral Disc Diseases: Causes, Diagnosis, Treatment and Prophylaxis. Thieme 2009.
- Laplante B., DePalma M.: Spine Osteoarthritis. American Academy of Physical Medicine and Rehabilitation 2012; 4: 28-36.
- Kalichman L., Hunter D.: Lumbar Facet Joint Osteoarthritis: A Review. Semin. Arthritis Rheum 2007; 37(2): 69-80.
- Solomon L., Warwick D., Nayagam S.: Apley’s System of Orthopaedics and Fractures. Hodder Arnold 2001.
- Kraemer J., Koester O.: MR Imaging of the Lumbar Spine. A Teaching Atlas. Thieme 2002.
- Kraemer R., Theodoridis T., Kraemer J.: Die lumbale Spinalkanalstenose. Springer 2011.
- Moore K.: Clinically Oriented Anatomy. Third Edition. Williams & Wilkins 1992.