Overview
Spondylolisthesis occurs when one vertebra slips over the adjacent one. It slides either forward (anterolisthesis) or backward (retrolisthesis). Spondylolisthesis manifests in different forms. The most common one is the isthmic or lytic spondylolisthesis, which also represents the most common cause of low back pain in adolescents.
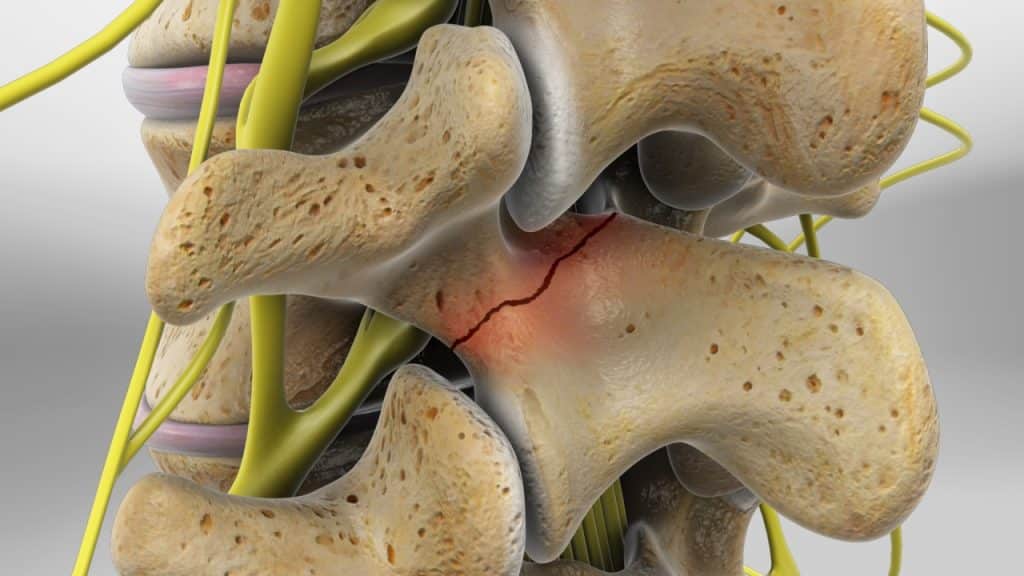
Spondylolysis is a small defect/crack in a portion of the spine known as pars interarticularis (bridge between two bones) which connects the superior and the inferior articular processes. It usually results from repeated stress to the bone (stress fracture). Spondylolysis most frequently occurs in young athletes who are involved in sports that require repeated hyperextension of the lower back (bending backwards) and usually affects both sides (bilateral manifestation).
Spondylolysis is the most common cause of isthmic spondylolisthesis and typically occurs at the L5-S1 level of the lumbar spine, where the L5 vertebral body slips over the sacrum. However, this does not necessarily mean that spondylolysis always leads to spondylolisthesis.
Anatomy (Lumbar anatomy)
The lumbar spine consists of five vertebrae which connect the sacrum (triangular bone at the bottom of the spine) to the thoracic spine (the upper back). All five vertebrae are numbered. The L1, the first lumbar vertebra, is closest to the thoracic spine. The L5, the lowest lumbar vertebra, is closest to the sacrum. The L stands for lumbar.
Anatomy (A typical lumbar vertebra)
A typical lumbar vertebra (bone of the spine) is composed of two parts. The vertebral body in the front (anterior) and the vertebral arch in the rear (posterior).
The vertebral arch encloses the vertebral foramen (opening). It consists of a pair of pedicles and a pair of laminae. At the junction of the pedicle and lamina on the right and left side, bony protrusions project upward and downward, known as superior and inferior articular processes.
The pars interarticularis (bridge between two bones) connects the superior and inferior articular processes. The pars interarticularis may also be referred to as the isthmus.
At the mid-point of the vertebral arch, a bony protrusion known as spinous process projects backward and downward. On either side of the spinous process, there are bony protrusions known as transverse processes. Similar to the spinous process, these processes provide attachments for ligaments and muscles.
The vertebrae (bones of the spine) articulate with one another at joints between their bodies and between their articular processes. The intervertebral discs provide the strongest attachment between the bodies of the vertebrae. In addition to the discs, the bodies are united by strong supporting ligaments.
Anatomy (Intervertebral discs)
The intervertebral discs are shock absorbers that are located between the bones of the spine, called vertebrae (hence the name intervertebral). They are designed to help the back stay flexible, while resisting forces and to allow bending, flexion and twisting of the spine. A healthy, well-hydrated disc contains a great amount of fluid in its centre, known as the nucleus pulposus, which provides cushioning and flexibility to the spine.
Anatomy (Facet joints)
The facet joints or zygapophyseal joints are a set of joints between the articular processes of two adjacent vertebrae. They are covered with cartilage and are surrounded by a lubricating capsule that enables the vertebrae to bend and twist. Each capsule has a rich supply of tiny nociceptive nerve fibers and implicates this structure as a potential source of pain. Similar to other joints in the body, these joints are vulnerable to inflammation and degeneration.
The facet joints provide support, stability and mobility to the vertebrae, especially on extending, bending and rotation. Furthermore, the articulation between the superior (above) and inferior (below) articular facets at the zygapophyseal joints as well as the intervertebral discs play an important role to prevent a vertebra slip over the adjacent one.
Isthmic or Lytic Spondylolisthesis
Isthmic or lytic spondylolisthesis is the most common cause of spondylolisthesis and typically occurs at the L5-S1 level of the lumbar spine, where the L5 vertebral body slips over the sacrum.
Spondylolysis is the most common cause of isthmic spondylolisthesis. It is a small defect/crack in a portion of the spine known as pars interarticularis (bridge between two bones) which connects the superior and the inferior articular processes. Pars interarticularis, also known as the isthmus, is a thin piece of bone with poor blood supply, which makes it vulnerable to stress fractures. Spondylolysis occurs most frequently in young athletes who are involved in sports that require repeated hyperextension of the lower back (bending backwards) and usually affects both sides (bilateral manifestation).
Low grade isthmic spondylolisthesis (slippage less than 10%) usually does not deteriorate after adulthood and does not predispose to low back pain at an older age. In contrast, high grade isthmic spondylolisthesis (slippage more than 25%) is highly associated with low back pain over time.
Symptoms
Spondylolisthesis and spondylolysis may be asymptomatic. The symptoms can be experienced in a variety of ways. Low back pain can be mild or so intense that the individual cannot follow everyday activities. It can occur suddenly or develop slowly and gradually aggravate over time. Low back pain usually gets worse after prolonged standing, walking or any type of activities that involves bending backwards and is often relieved by rest (sitting or lying down). Additionally, low back pain can be accompanied by pain, tingling, numbness and/or weakness that radiates from the lower back into the buttocks and legs in the area supplied by the affected nerve root (lumbar radiculopathy).
Treatment
Treatment for painful spondylolisthesis and spondylolysis focuses on minimizing pain, stabilizing the spine and improving or maintaining mobility. It can usually be treated successfully without surgery with a combination of rest, step positioning (stress-reducing positioning), heat therapy, analgesic/anti-inflammatory medications, orthopaedic braces and physical therapy.
Facet joint infiltrations or facet joint blocks may be administered not only to diagnose facet joint pain but also to treat it. If the patient shows a positive response to the facet joint blocks after having failed nonoperative care, the next treatment option is often radiofrequency denervation or rhizotomy.
The lumbar radiculopathy can usually be treated successfully without surgery with a combination of pain management techniques, physical therapy and therapeutic spinal injections.
Surgery may be recommended if the conservative therapies do not alleviate pain and the quality of life is still affected or if a significant neurologic deficit such as progressive muscle weakness exists. Surgery for spondylolisthesis usually comprises a decompression (also called a laminectomy) with or without spinal fusion with pedicle screw instrumentation (spondylodesis).
References
- Kraemer J., Hasenbring M., Kraemer R., Taub E., Theodoridis T., Wilke H.J.: Intervertebral Disc Diseases: Causes, Diagnosis, Treatment and Prophylaxis. Thieme 2009.
- Laplante B., DePalma M.: Spine Osteoarthritis. American Academy of Physical Medicine and Rehabilitation 2012; 4: 28-36.
- Kalichman L., Hunter D.: Lumbar Facet Joint Osteoarthritis: A Review. Semin. Arthritis Rheum 2007; 37(2): 69-80.
- Solomon L., Warwick D., Nayagam S.: Apley’s System of Orthopaedics and Fractures. Hodder Arnold 2001.
- Kraemer J., Koester O.: MR Imaging of the Lumbar Spine. A Teaching Atlas. Thieme 2002.
- Kraemer R., Theodoridis T., Kraemer J.: Die lumbale Spinalkanalstenose. Springer 2011.
- Moore K.: Clinically Oriented Anatomy. Third Edition. Williams & Wilkins 1992.