Overview
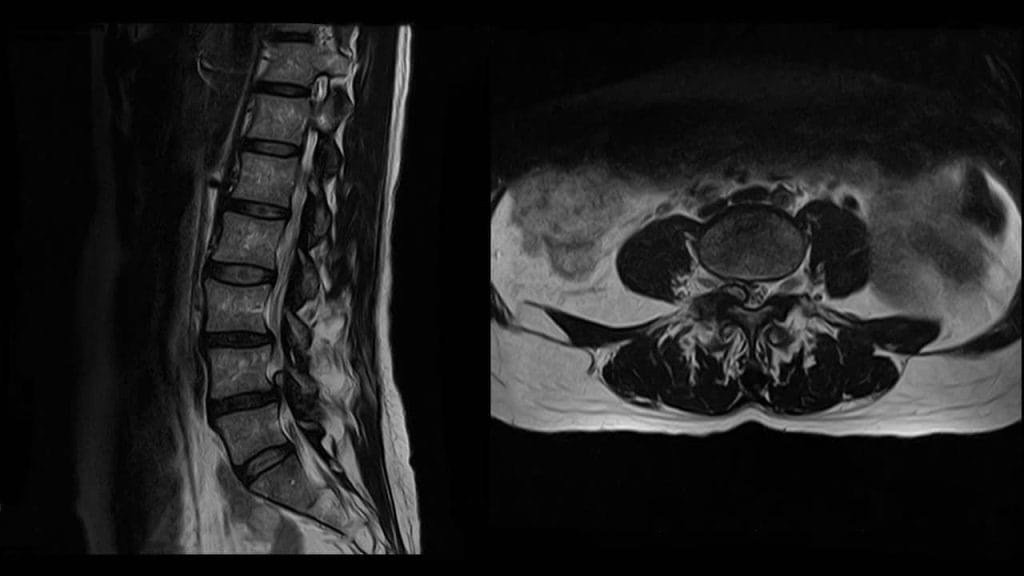
A synovial cyst is an abnormal fluid-filled sac that develops in the facet joints of the spine. This condition is commonly caused by age-related degeneration in the facet joints, a set of joints between the articular processes of two adjacent vertebrae. It typically occurs at the L4-L5 level of the lumbar spine (rarely at L3-L4 level) and it mostly affects people over 50. A synovial cyst may be asymptomatic and found incidentally or the fluid-filled sac creates pressure inside the spinal canal (bone channel occupied by the spinal nerves or the spinal cord) and may cause spinal stenosis with associated clinical symptoms. These include pain, tingling, numbness and/or weakness that radiates from the lower back into the buttocks and legs in the area supplied by the affected nerve root. A synovial cyst is best diagnosed by magnetic resonance imaging (MRI).
Anatomy (Facet joints)
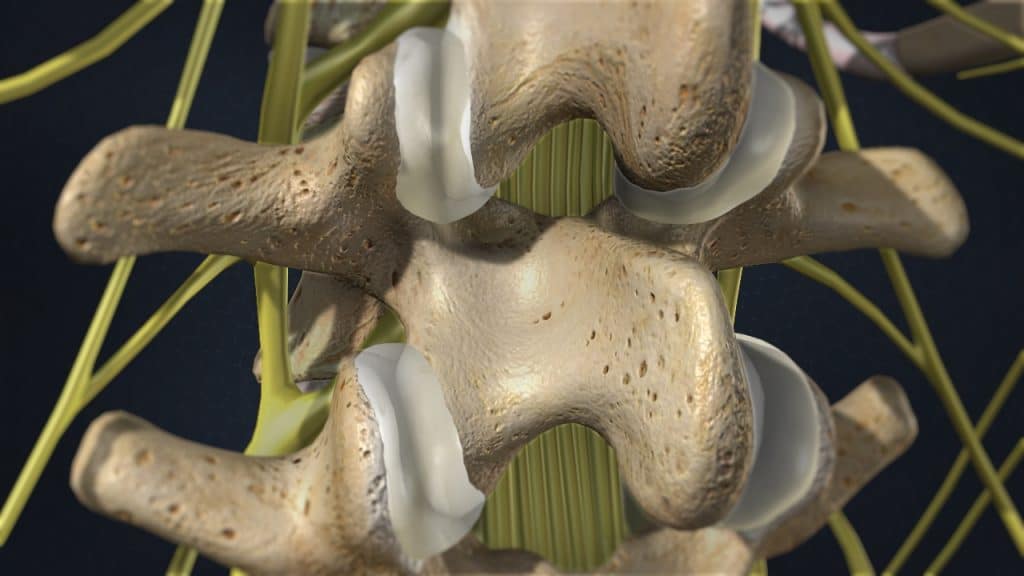
The facet joints or zygapophyseal joints are a set of joints between the articular processes of two adjacent vertebrae. They provide support, stability and mobility to the vertebrae, especially on extending, bending and rotation. Similar to other joints in the body, these joints are vulnerable to inflammation and degeneration.
The facet joints are covered with cartilage and are surrounded by a lubricating capsule that enables the vertebrae to bend and twist. Each capsule has a rich supply of tiny nociceptive nerve fibers that implicates this structure as a potential source of pain.
Anatomy (Synovial joint)
A synovial joint is a freely movable joint. The ends of the adjoining bones are covered with cartilage, a smooth, very slippery surface that permits a joint to move. A thick capsule surrounds the entire joint, lined with synovial membrane. The synovial membrane secretes a substance into the joint, called synovial fluid, which lubricates the joint, supplies with nutrients and oxygen the cartilage and removes the metabolic wastes.
Anatomy (Synovial Cyst)
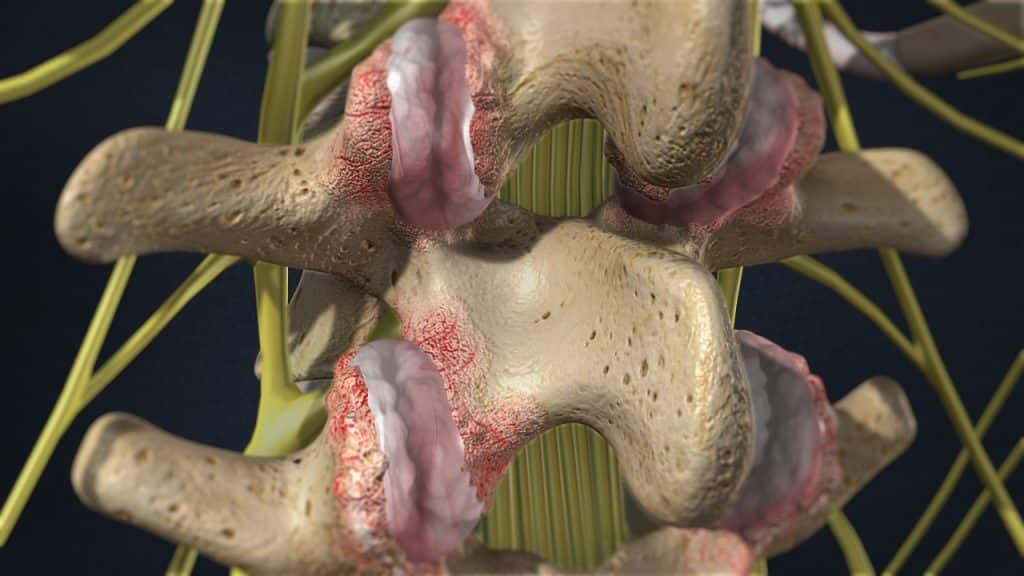
Joint degeneration may lead to excess synovial fluid production in attempt to keep the joint moving smoothly. It is thought that the synovial cyst develops as a result of this extra synovial fluid formation. When the fluid escapes from the degenerated, inflamed facet joint, because it is under pressure, it dilatates the joint capsule and creates a cyst. Such a cyst is also typical in the hollow of the knee, known as Baker cyst.
Anatomy (Spinal canal)
The entire length of the vertebral column has a large central canal or passage, called the spinal canal. In the cervical and thoracic regions of the spine, the spinal cord descends through this space. In the lumbar region of the spine, this space contains a bundle of nerve roots. Openings or holes to each side of the canal, called the neural foramen (intervertebral foramen – foramen between the two adjacent vertebrae) provide pathways for the nerve roots that travel from the spine to other parts of the body.
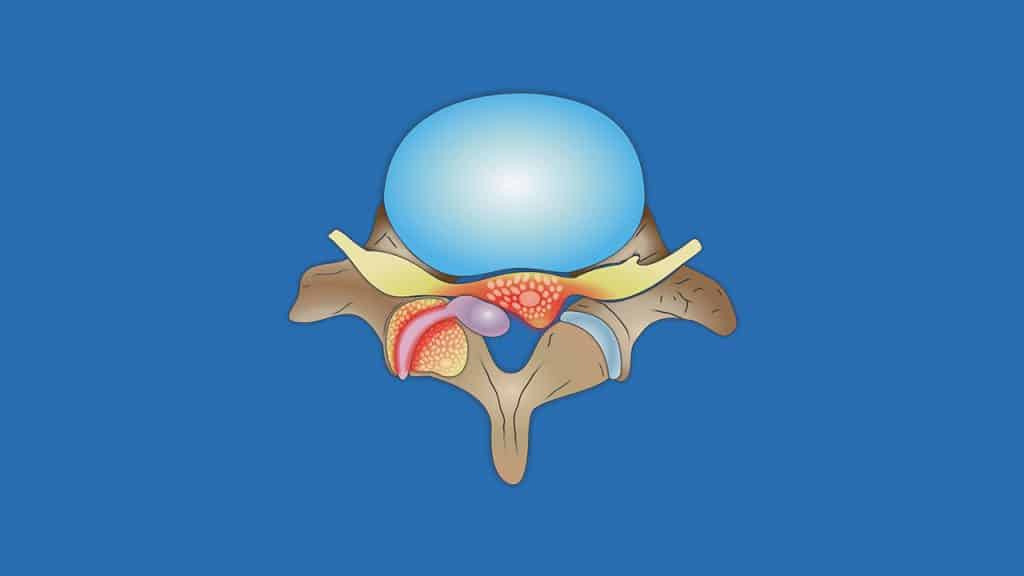
Stenosis
Normally, there is plenty of room for the nerves in the spinal canal and for the nerve roots as they exit the spine through the neural foramen. With spinal stenosis, however, the space for the spinal cord and/or the spinal nerves is constricted. The spinal nerves can become compressed against the vertebral bone. This can interfere with nerve function.
Symptoms
A synovial cyst may be asymptomatic. The symptoms depend on the size and location of the cyst and how it is impacting the surrounding neural structures.
In case of spinal stenosis in the lumbar region as a result of a synovial cyst, symptoms usually occur during certain activities such as walking (leg pain during walking known as claudication) and standing upright. They are often relieved by rest (sitting or lying down) and/or any flexed forward position, as this position opens up the spinal canal.
Spinal stenosis in the lower back commonly causes pain, tingling, numbness and/or weakness that radiates from the lower back into the buttocks and legs, in the area supplied by the affected nerve root. In rare cases, the severe compression on the nerve bundle at the end of the spinal cord, known as cauda equina (horse’s tail) can lead to serious problems such as a loss of bowel or bladder function, a condition known as cauda equina syndrome.
Spontaneous Resolution of Synovial Cysts
Spontaneous resolution of symptomatic synovial cyst has been reported in the literature. Resolution of a lumbar synovial cyst may generally be attributed to decreased inflammatory fluid production and decreased microtraumatic events or mechanical irritation of the cyst wall that results in extrusion of cyst contents and resolution of the cyst capsule.
Treatment
Treatment for painful synovial cyst focuses on alleviating pain, stabilizing the spine and improving or maintaining mobility. The extensive conservative treatment should always be considered as the first therapeutic option. This includes a combination of rest, step positioning (stress-reducing positioning), heat therapy, analgesic/anti-inflammatory medications, orthopaedic braces and physical therapy.
Facet joint infiltrations or epidural steroid injections may be administered in order to reduce pain and inflammation. Percutaneous cyst aspiration under CT-guidance and fluoroscopy or CT-guided percutaneous facet cyst distension and rupture might be additional therapeutical options.
Surgery may be recommended when conservative therapies do not alleviate pain and the quality of life is still affected or if a significant neurologic deficit such as progressive muscle weakness arises. Cauda equina syndrome is a medical emergency that calls for urgent surgical intervention.
Surgery for synovial cyst usually includes a resection and decompression (also called a hemi-/laminectomy) with or without spinal fusion with pedicle screw instrumentation (spondylodesis). Synovial cysts may reoccur following surgery.
References
- Kraemer R., Theodoridis T., Kraemer J.: Die lumbale Spinalkanalstenose. Springer 2011.
- Kraemer J., Koester O.: MR Imaging of the Lumbar Spine. A Teaching Atlas. Thieme 2002.
- Weyreuther M., Heyde C., Westphal M., Zierski J., Weber U.: MRT Atlas. Orthopädie und Neurochirurgie. Wirbelsäule. Springer 2005.
- Moore K.: Clinically Oriented Anatomy. Third Edition. Williams & Wilkins 1992.
- Krämer R., Herdmann J., Krämer J.: Mikrochirurgie der Wirbelsäule. Thieme 2005.
- Laplante B., DePalma M.: Spine Osteoarthritis. American Academy of Physical Medicine and Rehabilitation 2012; 4: 28-36.
- Kalichman L., Hunter D.: Lumbar Facet Joint Osteoarthritis: A Review. Semin. Arthritis Rheum 2007; 37(2): 69-80.
- Khan A.M., Girardi F.: Spinal lumbar synovial cysts. Diagnosis and management challenge. Review article. European Spine Journal 2006; 15: 1176-1182.
- Swartz P.G., Reed Murtagh F.: Spontaneous Resolution of an Intraspinal Synovial Cyst. American Journal Neuroradiology June/July 2003; 24: 1261-1263.
- Sinha P., Panbehcsi S., Lee Ming-Te, Parekh T., Pal D.: Spontaneous Resolution of Symptomatic Lumbar Synovial Cyst. Journal of Surgical Case Reports 2016; 2016(10): rjw 166.
- Ewald C., Kalff R.: Resolution of a synovial cyst of the lumbar spine without surgical therapy. A case report. Zentralbl Neurochir 2005; 66(3): 147-51.
- Epstein N., Baisden J.: The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int 17-Jul-2012;3.